|
Overview
 Fallen arches is one way of describing a flat or pronated foot. This can sometimes be implicated in ongoing problems such as lower back pain, knee pain, ankle pain, shin pain etc. The reason for the pronated foot is often due to the alignment of the bones within the foot, but can be increased by such things as ligament laxity, high body weight and a number of other specific conditions. One of these is posterior tibial dysfunction. This is a progressive disorder which allows the foot to pronate or lower on the inside section and can, if left untreated, result in quite debilitating effects. Causes As children grow, their legs will experience developmental changes that can result in excess flattening of the arches with weight bearing. One example is genu valgum, or knock-knees, a usually normal, temporary condition in children at different stages of growth. A tight calf muscle or Achilles tendon can also contribute to a flat foot. Many children will experience tight calf muscles as they go through growth spurts. Conditions that are present at birth and are often diagnosed early include: metatarsus adductus, calcaneovalgus and congenital vertical talus. Tarsal coalitions are congenitally fused foot bones that cause a rigid flat foot often associated with painful muscle spasms. This type of flat foot is usually diagnosed later in childhood or in adulthood. Any condition that causes loose ligaments can result in a flat foot or lower-than-normal arch. Ligaments are bands of tissue that connect bones to each other and have an important role in giving form to foot arches. An example of a condition that causes loosening of ligaments is pregnancy, where normal hormonal changes relax the ligaments. Diseases that cause loose ligaments include Ehlers-Danlos syndrome, Marfan's syndrome and rheumatoid arthritis. If one leg is longer than the other, one foot may be flat in relation to the other to compensate. Usually the foot on the longer limb will have a flatter arch in an effort to shorten that limb, balancing-out the unevenness. Leg length inequality can be caused by spinal abnormalities such as scoliosis. It can also be due to an actual difference in length of one leg bone compared to the other. Symptoms Having flat feet can be painless and is actually normal in some people. But others with flat feet experience pain in the heel or arch area, difficulty standing on tiptoe, or have swelling along the inside of the ankle. They may also experience pain after standing for long periods of time or playing sports. Some back problems can also be attributed to flat feet. Diagnosis An examination of the foot is enough for the health care provider to diagnose flat foot. However, the cause must be determined. If an arch develops when the patient stands on his or her toes, the flat foot is called flexible and no treatment or further work-up is necessary. If there is pain associated with the foot or if the arch does not develop with toe-standing, x-rays are necessary. If a tarsal coalition is suspected, a CT scan is often ordered. If a posterior tibial tendon injury is suspected, your health care provider may recommend an MRI. What causes pes planus? Non Surgical Treatment Most flexible flat feet are asymptomatic, and do not cause pain. In these cases, there is usually no cause for concern, and the condition may be considered a normal human variant. Flat feet were formerly a physical-health reason for service-rejection in many militaries. However, three military studies on asymptomatic adults (see section below), suggest that persons with asymptomatic flat feet are at least as tolerant of foot stress as the population with various grades of arch. Asymptomatic flat feet are no longer a service disqualification in the U.S. military. Surgical Treatment  Surgery for flat feet is separated into three kinds: soft tissue procedures, bone cuts, and bone fusions. Depending on the severity of the flat foot, a person?s age, and whether or not the foot is stiff determines just how the foot can be fixed. In most cases a combination of procedures are performed. With flexible flat feet, surgery is geared at maintaining the motion of the foot and recreating the arch. Commonly this may involve tendon repairs along the inside of the foot to reinforce the main tendon that lifts the arch. When the bone collapse is significant, bone procedures are included to physically rebuild the arch, and realign the heel. The presence of bunions with flat feet is often contributing to the collapse and in most situations requires correction. With rigid flat feet, surgery is focused on restoring the shape of the foot through procedures that eliminate motion. In this case, motion does not exist pre-operatively, so realigning the foot is of utmost importance. The exception, are rigid flat feet due to tarsal coalition (fused segment of bone) in the back of the foot where freeing the blockage can restore function. Overview
 Every time you take a step, one of your heels has to support the whole weight of your body. As you move, the load is equal to 20 times your own body weight. The load is softened by a pillow of fat under the heel and a large sinew or ligament (the fibrous tissue that joins muscle and bone together) under the sole of the foot. This sinew is called the plantar fascia and it pulls the heel bone forward (in opposition to the Achilles tendon, which pulls it backwards). If an athlete does not warm up properly or a person with a sedentary job exercises heavily during the weekends, they might overload the muscles of the calf or strain the Achilles tendon, which joins these muscles to the heel bone. When overloaded the tendon becomes tight and painfully inflamed, which places extra strain on the plantar fascia and muscles in the soles of the foot. The strained plantar fascia becomes inflamed and may even develop tiny cracks. This is known as plantar fasciitis. Every time you sit down, sleep or otherwise rest your legs, the muscles of the sole of the foot will contract in an attempt to protect the damaged sinew. The pain in the heel will then no longer be felt. But when you get up again and put weight on the foot, the foot and ankle may feel stiff (because of the inflammation) and the pain will return either at the back of the heel or on the soles of the feet. When you start to move, the plantar fascia may crack even more causing a vicious cycle of damage and pain. Inflammation at the point where the Achilles tendon (at the back of the heel) or the plantar fascia (under the heel) join the heel bone (a bone known as the Calcaneum) stimulates cells that form bone to deposit bone in this area, eventually leading to the build up of a bony prominence on the heel bone called a calcaneal spur. But it's not the spur itself that causes the pain. The spur is a sign of chronic inflammation in the connective tissues, which is the result of a prolonged overload. It should also be pointed out that heel spurs can occur on their own, without plantar fasciitis or pain, or may be linked to some types of arthritis (inflammation of the joints). And plantar fasciitis or Achilles tendonitis don't necessarily lead to spur formation. Causes If it hurts under your heel, you may have one or more conditions that inflame the tissues on the bottom of your foot. When you step on a hard object such as a rock or stone, you can bruise the fat pad on the underside of your heel. It may or may not look discolored. The pain goes away gradually with rest. Doing too much running or jumping can inflame the tissue band (fascia) connecting the heel bone to the base of the toes. The pain is centered under your heel and may be mild at first but flares up when you take your first steps after resting overnight. You may need to do special exercises, take medication to reduce swelling and wear a heel pad in your shoe. When plantar fasciitis continues for a long time, a heel spur (calcium deposit) may form where the fascia tissue band connects to your heel bone. Your doctor may take an X-ray to see the bony protrusion. Treatment is usually the same as for plantar fasciitis: rest until the pain subsides, do special stretching exercises and wear heel pad shoe inserts. Having a heel spur may not cause pain and should not be operated on unless symptoms become chronic. Symptoms Initially, this pain may only be present when first standing up after sleeping or sitting. As you walk around, the muscle and tendon loosen and the pain goes away. As this problem progresses, the pain can be present with all standing and walking. You may notice a knot or bump on the back of the heel. Swelling may develop. In some cases, pressure from the back of the shoe causes pain. Diagnosis A biomechanical exam by your podiatrist will help reveal these abnormalities and in turn resolve the cause of plantar fasciitis. By addressing this cause, the patient can be offered a podiatric long-term solution to his problem. Non Surgical Treatment Home care, in cases that are not severe, home care is probably enough to get rid of heel pain. Rest, avoid running or standing for long periods, or walking on hard surfaces. Avoid activities that may stress the heels. Ice, place an ice-pack on the affected area for about 15 minutes. Do not place bare ice directly onto skin. Footwear. proper-fitting shoes that provide good support are crucial. Athletes should be particularly fussy about the shoes they use when practicing or competing - sports shoes need to be replaced at specific intervals (ask your trainer). Foot supports, wedges and heel cups can help relieve symptoms. Surgical Treatment At most 95% of heel pain can be treated without surgery. A very low percentage of people really need to have surgery on the heel. It is a biomechanical problem and it?s very imperative that you not only get evaluated, but receive care immediately. Having heel pain is like having a problem with your eyes; as you would get glasses to correct your eyes, you should look into orthotics to correct your foot. Orthotics are sort of like glasses for the feet. They correct and realign the foot to put them into neutral or normal position to really prevent heel pain, and many other foot issues. Whether it be bunions, hammertoes, neuromas, or even ankle instability, a custom orthotic is something worth considering. heelsncleavage Prevention  You can try to avoid the things that cause heel pain to start avoid becoming overweight, where your job allows, minimise the shock to your feet from constant pounding on hard surfaces, reduce the shocks on your heel by choosing footwear with some padding or shock-absorbing material in the heel, if you have high-arched feet or flat feet a moulded insole in your shoe may reduce the stresses on your feet, if you have an injury to your ankle or foot, make sure you exercise afterwards to get back as much movement as possible to reduce the stresses on your foot and your heel in particular, If you start to get heel pain, doing the above things may enable the natural healing process to get underway and the pain to improve. Overview
Shortening techniques can be used after skeletal maturity to achieve leg length equality. Shortening can be done in the proximal femur using a blade plate or hip screw, in the mid-diaphysis of the femur using a closed intramedullary (IM) technique, or in the tibia. Shortening is an accurate technique and involves a much shorter convalescence than lengthening techniques. Quadriceps weakness may occur with femoral shortenings, especially if a mid-diaphyseal shortening of greater than 10% is done. If the femoral shortening is done proximally, no significant weakness should result. Tibial shortening can be done, but there may be a residual bulkiness to the leg, and risks of nonunion and compartment syndrome are higher. If a tibial shortening is done, shortening over an IM nail and prophylactic compartment release are recommended. We limit the use of shortenings to 4 to 5 cm leg length inequality in patients who are skeletally mature.  Causes The causes of LLD may be divided into those that shorten a limb versus those that lengthen a limb, or they may be classified as affecting the length versus the rate of growth in a limb. For example, a fracture that heals poorly may shorten a leg slightly, but does not affect its growth rate. Radiation, on the other hand, can affect a leg's long-term ability to expand, but does not acutely affect its length. Causes that shorten the leg are more common than those that lengthen it and include congenital growth deficiencies (seen in hemiatrophy and skeletal dysplasias ), infections that infiltrate the epiphysis (e.g. osteomyelitis ), tumors, fractures that occur through the growth plate or have overriding ends, Legg-Calve-Perthes disease, slipped capital femoral epiphysis (SCFE), and radiation. Lengthening can result from unique conditions, such as hemihypertrophy , in which one or more structures on one side of the body become larger than the other side, vascular malformations or tumors (such as hemangioma ), which cause blood flow on one side to exceed that of the other, Wilm's tumor (of the kidney), septic arthritis, healed fractures, or orthopaedic surgery. Leg length discrepancy may arise from a problem in almost any portion of the femur or tibia. For example, fractures can occur at virtually all levels of the two bones. Fractures or other problems of the fibula do not lead to LLD, as long as the more central, weight-bearing tibia is unaffected. Because many cases of LLD are due to decreased rate of growth, the femoral or tibial epiphyses are commonly affected regions. Symptoms LLD do not have any pain or discomfort directly associated with the difference of one leg over the other leg. However, LLD will place stress on joints throughout the skeletal structure of the body and create discomfort as a byproduct of the LLD. Just as it is normal for your feet to vary slightly in size, a mild difference in leg length is normal, too. A more pronounced LLD, however, can create abnormalities when walking or running and adversely affect healthy balance and posture. Symptoms include a slight limp. Walking can even become stressful, requiring more effort and energy. Sometimes knee pain, hip pain and lower back pain develop. Foot mechanics are also affected causing a variety of complications in the foot, not the least, over pronating, metatarsalgia, bunions, hammer toes, instep pain, posterior tibial tendonitis, and many more. Diagnosis On standing examination one iliac crest may be higher/lower than the other. However a physiotherapist, osteopath or chiropractor will examine the LLD in prone or supine position and measure it, confirming the diagnosis of structural (or functional) LLD. The LLD should be measured using bony fixed points. X-Ray should be taken in a standing position. The osteopath, physiotherapist or chiropractor will look at femoral head & acetabulum, knee joints, ankle joints. Non Surgical Treatment Non-surgical treatment can be effective. A shoe lift may be recommended if the leg length difference is less than 1 inch. More significant leg length discrepancies may require a surgical procedure. In children, surgical procedures are available to help make leg lengths more equal.  how to increase height naturally after 21 Surgical Treatment The bone is lengthened by surgically applying an external fixation device to the leg. The external fixator, a scaffold-like frame, is connected to the bone with wires, pins, or both. A small crack is made in the bone and the frame creates tension when the patient or family member turns its dial. This is done several times each day. The lengthening process begins approximately five to 10 days after surgery. The bone may lengthen 1 millimeter per day, or approximately 1 inch per month. Lengthening may be slower in a bone that was previously injured. It may also be slower if the leg was operated on before. Bones in patients with potential blood vessel abnormalities, such as cigarette smokers, may also need to be lengthened more slowly. The external fixator is worn until the bone is strong enough to support the patient safely. This usually takes about three months for each inch. Factors such as age, health, smoking and participation in rehabilitation can affect the amount of time needed. Overview
 A Morton's neuroma usually develops between the third and fourth toes. Less commonly, it develops between the second and third toes. Other locations are rare. It also is rare for a Morton's neuroma to develop in both feet at the same time. The condition is much more common in women than men, probably as a result of wearing high-heeled, narrow-toed shoes. This style of shoe tends to shift the bones of the feet into an abnormal position, which increases the risk that a neuroma will form. Being overweight also increases the risk of a Morton's neuroma. A Morton's neuroma usually develops between the third and fourth toes. Less commonly, it develops between the second and third toes. Other locations are rare. It also is rare for a Morton's neuroma to develop in both feet at the same time. The condition is much more common in women than men, probably as a result of wearing high-heeled, narrow-toed shoes. This style of shoe tends to shift the bones of the feet into an abnormal position, which increases the risk that a neuroma will form. Being overweight also increases the risk of a Morton's neuroma.Causes There are orthoses and corrective shoes that can effectively alleviate disturbances to foot mechanics. A podiatric physician can prescribe the best corrective footwear and shoe inserts for all activities, work, exercise, play, walking, shopping and more, based on an analysis of the patient?s foot and his or her lifestyle. Improper footwear. Podiatric physicians have long believed that constricting, narrow, poor-fitting shoes with a tight or pointed toe box tend to compress the end of the foot, leading to abnormal motion of the foot and to excessive pressure in the area of the nerve. High-heeled shoes are a particular culprit here, since they put pressure on the area around wearer?s toes and the ball of the foot. Symptoms Pain is usually increased by forefoot weight bearing activities (such as running), with narrow-fitting footwear, or with high heeled shoes. It is usually painful to firmly touch the affected region and, in chronic cases, pain and sometimes an audible click, may be heard when squeezing the foot and toes together with the hand. Often a localized area of swelling may be evident at the site of injury. Diagnosis To confirm the diagnosis, your doctor will examine your feet. He or she will look for areas of tenderness, swelling, calluses, numbness, muscle weakness and limited motion. To check for a Morton's neuroma, your doctor will squeeze the sides of your foot. Squeezing should compress the neuroma and trigger your typical pain. In some cases, your doctor will find numbness in the webbed area between the affected toes. Pain in two or more locations on one foot, such as between both the second and third toes and the third and fourth toes, more likely indicates that the toe joints are inflamed rather than a Morton' neuroma. Non Surgical Treatment The first line of treatment is to try modifying footwear. Often simply wearing broader fitting shoes can reduce pressure on the neuroma and so reduce pain. Orthotic inserts can also help as they can again help reduce pressure on certain parts of the foot. Padding and taping the toe area is another option. In some cases a steroid injection into the foot may be suggested. This can be done as a day case without the need for anaesthesia and helps reduce inflation of the nerve. It can halt the pain in round 70 % of cases. Sometimes a combination of alcohol and local anaesthesia may be injected as this helps reduce pain.  Surgical Treatment If symptoms do not respond to any of the above measures then surgery may be suggested. This involves a short 30 minute operation to either remove tissue to take pressure off the nerve or to remove the nerve causing the pain. The surgery can be done as a day case but it will be two or three weeks before you can be fully active on your feet. There may be some lingering numbness afterwards if the nerve is removed. But surgery is successful in around 80% of cases. There is a small risk of complications such as infection and thickening of the skin on the soles of the feet. Prevention Ensuring that shoes are well fitted, low-heeled and with a wide toe area may help to prevent Morton's neuroma.  Overview OverviewThere are two main types of Hammertoe. Hammertoes can be flexible, which means that you can still move the toe a bit - these are easier to treat with stretching, wider shoes and in some cases, toe splints. Rigid hammertoes occur when the foot condition has persisted for so long without treatment that the tendons become too rigid to be stretched back to normal. Rigid hammertoes are more common in people with arthritis. This foot condition usually needs to be treated with surgery. Causes Hammertoes are most common in women, and a big part of this is poor shoe choices, which are a big factor in the development of many foot problems. Tight toe boxes and high heels are the biggest culprits. Genetics certainly plays a role in some cases of hammertoes, as does trauma, infection, arthritis, and certain neurological and muscle disorders. But most cases of contracted toes are associated with various biomechanical abnormalities in how a patient walks. This causes the muscles and tendons to be used excessively or improperly, which deforms the toes over time.  Symptoms The most obvious sign of hammertoes are bent toes, other symptoms may include pain and stiffness during movement of the toe. Painful corns on the tops of the toe or toes from rubbing against the top of the shoe's toe box. Painful calluses on the bottoms of the toe or toes. Pain on the bottom of the ball of the foot. Redness and swelling at the joints. Diagnosis The earlier a hammertoe is diagnosed, the better the prognosis and treatment options. Your doctor will be able to diagnose your hammertoe with a simple examination of the foot and your footwear. He or she may take an x-ray to check the severity of the condition. You may also be asked about your symptoms, your normal daily activities, and your medical and family history. Non Surgical Treatment Symptomatic treatment of hammertoes consists of such things as open toed shoes or hammertoe pads. There are over the counter corn removers for temporally reducing the painful callous often seen with the hammertoe. These medications must be used with caution. They are a mild acid that burns the callous off. These medications should never be used for corns or callouses between the toes. Persons with diabetes or bad circulation should never use these products. Surgical Treatment Surgical correction is needed to bring the toe into a corrected position and increase its function. Correction of the hammer toes is a simple outpatient surgery, with limited downtime. The best option is to fuse the deformed and contracted toe into a straight position. This limits the need for future surgery and deformity return. A new pin that absorbs in the bone or small screw is used by the Foot and Ankle Institute to avoid the need for a metal pin protruding from the toe during recovery. Although the absorbable pin is not for everyone, it is much more comfortable than the pin protruding from the end of the toe. In certain cases, a removal of a small area of bone in the deformity area will decrease pain and limit the need for a surgical waiting period that is found with fusions. Although the toe is not as stable as with a fusion, in certain cases, an arthroplasty is the best option.  Prevention Preventative treatment of hammertoe is directed toward the cause of the deformity. A functional orthotic is a special insert that can be prescribed by your podiatrist to address the abnormal functioning of the foot that causes the hammertoe. Functional orthotics can be thought of as contact lenses for your feet. They correct a number of foot problems that are caused by an abnormally functioning foot. Our feet, much like our eyes, change with time. Functional orthotics slow down or halt this gradual change in the foot. Often when orthotics are used for flexible hammertoes, the toes will overtime straighten out and correct themselves. Calf stretching exercises are also helpful. Calf stretching can help to overcome part of the muscle imbalance that causes the hammertoe.
Overview
 A bunion (Hallux Abducto Valgus) is sometimes described as a bump on the side of the big toe. However, the visible bump actually reflects changes in the bony framework in the front part of the foot. Instead of pointing straight ahead, the big toe leans towards the second toe, throwing the bones out of alignment and producing the ?bump? of the bunion. Bunions are a progressive disorder and gradually change the angle of the bones in your foot over the years. Symptoms usually occur in the later stages. The skin over the base of your big toe may become red and tender, and make wearing shoes painful. The bigger the bunion gets, the more it hurts to walk. Pressure from your big toe can force your second toe out of alignment, sometimes overlapping your third toe. Severe bunions can make it difficult to walk and you may develop arthritis. A bunion (Hallux Abducto Valgus) is sometimes described as a bump on the side of the big toe. However, the visible bump actually reflects changes in the bony framework in the front part of the foot. Instead of pointing straight ahead, the big toe leans towards the second toe, throwing the bones out of alignment and producing the ?bump? of the bunion. Bunions are a progressive disorder and gradually change the angle of the bones in your foot over the years. Symptoms usually occur in the later stages. The skin over the base of your big toe may become red and tender, and make wearing shoes painful. The bigger the bunion gets, the more it hurts to walk. Pressure from your big toe can force your second toe out of alignment, sometimes overlapping your third toe. Severe bunions can make it difficult to walk and you may develop arthritis.Causes Bunions are among the most common problems of the foot. They are several possible reasons a bunion may develop, though a biomechanical abnormality (improper function of the foot) is the most common cause. In an unstable flat foot, for example, a muscular imbalance often develops that, over time, causes bunions. Bunions tend to run in families, and most podiatrists believe that genetic factors play a role in predisposing some people to develop bunions. Poor shoes, like high heels and pointed toe boxes--exacerbate the condition by speeding up the development of bunions, and by making bunions more painful. Poor shoe choices is at least one of the reasons bunions are much more common in women than men. Symptoms The symptoms of a bunion include the following development of a firm bump on the outside edge of the foot, at the base of the big toe, redness, swelling, or pain at or near the MTP joint, corns or other irritations caused by the overlap of the first and second toes, restricted or painful motion of the big toe. Diagnosis Your doctor is very likely to be able to diagnose your bunion simply by examining your foot. Even before that, he or she will probably ask about your family and personal medical history and evaluate the types of shoes you wear. You'll be asked about your symptoms, when they started and when they occur. You may also be asked to flex your toe so that your doctor can get an idea of your range of motion. He or she may order x-rays in order to determine the extent of your deformity. Non Surgical Treatment Patients with a painful bunion may benefit from four to six physical therapy treatments. Your therapist can offer ideas of shoes that have a wide toe box (mentioned earlier). The added space in this part of the shoe keeps the metatarsals from getting squeezed inside the shoe. A special pad can also be placed over the bunion. Foot orthotics may be issued to support the arch and hold the big toe in better alignment. These changes to your footwear may allow you to resume normal walking immediately, but you should probably cut back on more vigorous activities for several weeks to allow the inflammation and pain to subside. Treatments directed to the painful area help control pain and swelling. Examples include ultrasound, moist heat, and soft-tissue massage. Therapy sessions sometimes include iontophoresis, which uses a mild electrical current to push anti-inflammatory medicine to the sore area. This treatment is especially helpful for patients who can't tolerate injections.  Surgical Treatment Depending on the size of the enlargement, misalignment of the toe, and pain experienced, conservative treatments may not be adequate to prevent progressive damage from bunions. In these cases, bunion surgery, known as a bunionectomy, may be advised to remove the bunion and realign the toe. Prevention Shop for shoes that possess a removable liner, or insole, and stand on the liner after you have removed it from your shoe. This is an effective method to see if your shoe is wide enough in the forefoot to accommodate your bunion. If your bunion and forefoot are wider than the insole, your shoe will squeeze and constrict your bunion and create the symptoms that define this health problem. The insole should also be wide enough to fully accommodate your big toe when it points outward, away from your other toes. Overview
Pronation, in anatomical terms, means to rotate, and it applies to any rotational movement of a bone. Pronation in the feet involves an inward rolling of the foot throughout the gait which helps with the transfer of force. Normally the foot will move from the heel to the toes with only a small degree of pronation, with a slight inward roll from the outside of the heel to the inside of the foot which helps to support the body weight. Normal pronation involves the rolling of the foot to approximately 15 degrees. If you have normal foot arches, you are likely to be a neutral runner and will most likely pronate normally.  Causes Flat feet don't automatically mean you have a problem. The problem can be divided into a flexible flat foot or rigid flat foot. The rigid flat foot is one that does not change shape when the foot becomes weight bearing. i.e. it does not go through the excessive motion of pronation. Generally speaking this foot does not provide too many problems. The flexible flat foot is the type that when it becomes weight bearing the foot and ankle tends to roll in (pronates) too far. This type of person will often say I have great arches but when I stand up much of this arch disappears as the foot excessively pronates When the foot is excessively pronating and causing problems like sore ankles, feet or knees when standing or exercising then arch support is extremely important to restore the foot structure. Symptoms Overpronation can be a contributing factor in other lower extremity disorders, such as foot pain, plantar fasciitis, ankle injuries, medial tibial stress syndrome (shin splints), periostitis, stress fractures and myofascial trigger points. Overpronation increases the degree of internal tibial rotation, thereby contributing to various knee disorders such as meniscal injury or ligament sprains. The effects of the postural deviation are exaggerated in athletes due to the increase in foot strikes while running and the greater impact load experienced. When running, three to four times the body weight is experienced with each foot strike.2 If overpronation exists, the shock force is not adequately absorbed by the foot and is transmitted further up the kinetic chain. Diagnosis A quick way to see if you over-pronate is to look for these signs. While standing straight with bare feet on the floor, look so see if the inside of your arch or sole touches the floor. Take a look at your hiking or running shoes; look for wear on the inside of the sole. Wet your feet and walk on a surface that will show the foot mark. If you have a neutral foot you should see your heel connected to the ball of your foot by a mark roughly half of width of your sole. If you over-pronate you will see greater than half and up to the full width of your sole.  Non Surgical Treatment Anti-Pronation Insoles provide a unique foot support system that aligns the lower body. The major cause of foot and leg pain is over pronation (rolling over of the feet) which causes excessive pressure on the muscles, ligaments and bones of the lower body. Running insoles treat the underlying cause of over pronation and prevent future occurrences of the associated foot or leg condition. A project conducted at the NIKE Sport Research Laboratory studied the effects of orthotics on rear foot movement in running. Nine well-trained runners who wore orthotics were chosen as subjects. The results of the study indicated that orthotics reduced rear foot movement by roughly one degree or approximately nine percent of the amount found in runners not using orthotics. The average reduction of the maximum velocity of pronation was fifteen percent. Thus this study indicates that orthotics and insoles control over pronation which will treat and prevent many sporting injuries. Surgical Treatment The MBA implant is small titanium device that is inserted surgically into a small opening between the bones in the hind-mid foot: the talus (ankle bone) and the calcaneus (heel bone). The implant was developed to help restore the arch by acting as a mechanical block that prevents the foot from rolling-in (pronation). In the medical literature, the success rate for relief of pain is about 65-70%. Unfortunately, about 40% of people require surgical removal of the implant due to pain. Overview
A common cause of heel pain in growing adolescents, particularly those that are actively participating in sport is a condition known as Severs disease. While the suggestion of a ?disease? to your child may conjure up images of a life threatening disorder crippling your child, Severs disease is not nearly so sinister and can be easily fixed. Causes Growth plates, also called epiphyseal plates, occur at the end of long bones in children who are still growing. These plates are at either end of growing bones, and are the place where cartilage turns into bone. As children grow, these plates eventually become bone (a process called ossification). During a growth spurt, the bone in the heel may outpace the growth of the muscles and tendons that are attached to the heel, such as the Achilles tendon. During weight bearing, the muscles and tendons begin to tighten, which in turn puts stress on the growth plate in the heel. The heel is not very flexible, and the constant pressure on it begins to cause the symptoms of Sever?s disease. Sever?s disease is common, and it does not predispose a child to develop any other diseases or conditions in the leg, foot, or heel. It typically resolves on its own. Symptoms Patients with Severs disease typically experience pain that develops gradually in the back of the heel or Achilles region. In less severe cases, patients may only experience an ache or stiffness in the heel that increases with rest (especially at night or first thing in the morning). This typically occurs following activities which require strong or repetitive contraction of the calf muscles, such as running (especially uphill) or during sports involving running, jumping or hopping. The pain associated with this condition may also warm up with activity in the initial stages of the condition. As the condition progresses, patients may experience symptoms that increase during activity and affect performance. Pain may also increase when performing a calf stretch or heel raise (i.e. rising up onto tip toes). In severe cases, patients may walk with a limp, have difficulty putting their heel down, or be unable to weight bear on the affected leg. Pain may also increase on firmly touching the affected region and occasionally a bony lump may be palpable or visible at the back of the heel. This condition typically presents gradually overtime and can affect either one or both lower limbs. Diagnosis To diagnose the cause of the child?s heel pain and rule out other more serious conditions, the foot and ankle surgeon obtains a thorough medical history and asks questions about recent activities. The surgeon will also examine the child?s foot and leg. X-rays are often used to evaluate the condition. Other advanced imaging studies and laboratory tests may also be ordered. Non Surgical Treatment Depending on the diagnosis and the severity of the pain, there a number of treatment options available. Rest, reduce activity, your child should reduce or stop any activity that causes pain, such as sports and running. This can be a difficult option, as children are normally quite willful in pursuit of their favorite pastimes. Over the counter anti-inflammatory drugs, such as ibuprofen (found in Nurofen), to help reduce pain and inflammation. Make certain your child does stretching exercises before play. This will often help reduce the stress on the fascia and relieve heel pain in your child. Orthotic insoles. Orthotics made for children will help support the foot properly, and help prevent over-pronation or improper gait by supporting your child?s foot into a proper biomechanical position. Do not hesitate to schedule an appointment with a podiatrist, should your child?s heel and foot pain persist. Prevention Sever's disease may be prevented by maintaining good joint and muscle flexibility in the years leading up to, and during, their growth spurts (eg girls 8 to 10, boys 10 to 12). Foot arch problems such as flat feet should be addressed after the age of five if they don't appear to be self-correcting. If you are concerned, please ask your health practitioner. The most important factor is the amount of weight-bearing exercise your child is currently performing. Finally, LISTEN To Your Child! If your child is suffering heel pain between the ages of 8 to 12, suspect Sever's disease until proven otherwise. Seek the professional opinion of your foot practitioner regarding its diagnosis and subsequent management. Overview
Arch pain is commonly experienced by middle aged women who's feet have a tendency to overpronate or roll in. It is also commonly associated with bunions and hammer toe. The plantar plate is a thick ligament type structure with attachments which inserts into the base of our phalanges (toe bones) in the area of the ball of the foot. The plantar plate is designed to protect the head of the metatarsal from pressure and prevent over extension of our toes preventing our toes from spreading or splaying.  Causes There are several reasons why arch pain develops. Sometimes it?s due to a condition known as plantar fasciitis, in which the plantar fascia (the band of tissue that runs along the bottom of your foot from your heel to your toes) becomes inflamed after excessive stress. Heel pain results from this inflammation. Sometimes the pain is due to extensive time spent on your feet. Many people feel pain on the arch of their feet after a long workday, while others overuse their feet exercising or playing sports. A foot deformity, such as hammertoe or clubfoot, can also cause this pain. Medical conditions such as diabetes or obesity can put additional stress on your feet, thereby causing arch pain. Your footwear is also important. Shoes should support all parts of your foot, especially the bottom. This is very important if you spend excessive time on your feet, if your obese, if your pregnant, or if you engage in sport-related activities. Injuries to any of the twenty-six bones, thirty-three joints and over 100 muscles, tendons and ligaments in the feet can also cause arch pain. Because the foot is such a complex structure, it?s important to see a podiatrist at the first sign of symptoms. Symptoms Symptoms of plantar fasciitis may occur anywhere along the arch, but it is most common near its attachment to the heel bone. Symptoms of plantar fasciitis vary, but the classic symptom is pain after rest--when you first get out of bed in the morning, or when you get up after sitting down for a while during the day. This is known as "post-static dyskinesia." The pain usually diminishes after a few minutes of walking, sometimes even disappearing, but the pain is commonly felt again the longer you're on the foot. Fasciitis can be aggravated by shoes that lack appropriate support, especially in the arch area, and by the chronic irritation of long-periods of standing, especially on concrete, and by being overweight. Other factors which influence this condition are gender (females get this more than men), age (30s to 50s are most common), and those with flatter-than-normal feet. It doesn't help that fascia doesn't heal particularly quickly. This is because it has relatively poor circulation, which is why it's white in colour. Diagnosis Diagnosis of a plantar plate tear can often be challenging due to the complex nature of the anatomy of the foot. Careful history taking and an examination of the area of pain is required to determine the extent and cause of the tear. If necessary, further investigations such as x-rays or diagnostic ultrasound may be ordered by your podiatrist to help evaluate the severity of the problem. Non Surgical Treatment Just as there are many different causes of flat feet, there are also many different treatment options. The most important aspect of treatment is determining the exact type or underlying cause of flat feet that you have. Foot and ankle specialists can determine this through thorough clinical examination and special imaging studies (e.g., x-rays, computed tomography, and/or magnetic resonance imaging). Conservative treatment is effective in the vast majority of flat foot cases, and consists of things such as insoles, splints, manipulation, or casting. Surgery is required much less frequently, and is reserved only for some of the severe types of flat foot that do not respond to conservative therapy. 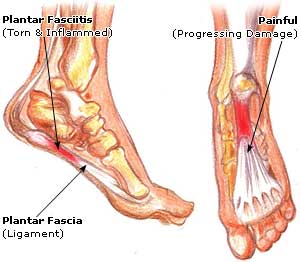 Surgical Treatment If pain or foot damage is severe, your doctor may recommend surgery. Procedures may include the following. Fusing foot or ankle bones together (arthrodesis). Removing bones or bony growths also called spurs (excision). Cutting or changing the shape of the bone (osteotomy). Cleaning the tendons' protective coverings (synovectomy). Adding tendon from other parts of your body to tendons in your foot to help balance the "pull" of the tendons and form an arch (tendon transfer). Grafting bone to your foot to make the arch rise more naturally (lateral column lengthening). Prevention There are several things you can do to prevent pain on the bottom of the foot. Here are some tips to help you avoid this condition. Do simple stretches each day (See Plantar Fasciitis Exercises for a list of all exercises). Wear good shoes that fit properly and are appropriate for the activity you are participating in. Lose excess weight if possible. Build your stamina slowly, especially with new exercises. Rest and elevate your feet, whenever possible, keeping them at least twelve inches above your heart. Always follow your doctor?s instructions for treatment. Each day do a different activity. For example: one day ride your bike, and swim the next day. Stretching Exercises Plantar Fasciitis stretches can be incorporated into a comprehensive treatment regime which may involve: ice, heel wedge support, taping, massage, muscle strengthening, orthotic inserts for shoes, topical anti inflammatory gel or oral medication and/or corticosteroid injections. If you suspect you may have Plantar Fasciitis seek accurate diagnosis and treatment from a health professional to ensure a correct diagnosis and reduce the likelihood of developing chronic foot pain. Treatment interventions may be provided by your Physical Therapist, Podiatrist and/or doctor.
Overview
 An Achilles tendon rupture, or tear, is a common condition. This typically occurs in the unconditioned individual who sustains the rupture while playing sports, or perhaps, from tripping. There is a vigorous contraction of the muscle and the tendon tears. Causes The tendon is susceptible to injury and can rupture during vigorous activities such as running and jumping. Rupture can also occur as a result of gradual wear. After becoming chronically weakened, it can rupture during non-stress activities like walking. Symptoms A sudden and severe pain may be felt at the back of the ankle or calf, often described as "being hit by a rock or shot" or "like someone stepped onto the back of my ankle." The sound of a loud pop or snap may be reported. A gap or depression may be felt and seen in the tendon about 2 inches above the heel bone. Initial pain, swelling, and stiffness may be followed by bruising and weakness. The pain may decrease quickly, and smaller tendons may retain the ability to point the toes. Without the Achilles tendon, though, this would be very difficult. Standing on tiptoe and pushing off when walking will be impossible. A complete tear is more common than a partial tear. Diagnosis During the physical exam, your doctor will inspect your lower leg for tenderness and swelling. In many cases, doctors can feel a gap in your tendon if a complete rupture has occurred. Achilles tendon rupture can be diagnosed reliably with clinical examination, but if there?s a question about the extent of your Achilles tendon injury then your doctor may order a magnetic resonance imaging (MRI) scan. Non Surgical Treatment Medical therapy for a patient with an Achilles tendon rupture consists of rest, pain control, serial casting, and rehabilitation to maximize function. Ongoing debate surrounds the issue of whether medical or surgical therapy is more appropriate for this injury. Conservative management of Achilles tendinosis and paratenonitis includes the following. Physical therapy. Eccentric exercises are the cornerstone of strengthening treatment, with most patients achieving 60-90% pain relief. Orthotic therapy in Achilles tendinosis consists of the use of heel lifts. Nonsteroidal anti-inflammatory drugs (NSAIDs). Tendinosis tends to be less responsive than paratenonitis to NSAIDs. Steroid injections. Although these provide short-term relief of painful symptoms, there is concern that they can weaken the tendon, leading to rupture. Vessel sclerosis. Platelet-rich plasma injections. Nitric oxide. Shock-wave therapy. An Achilles tendon rupture, or tear, is a common condition. This typically occurs in the unconditioned individual who sustains the rupture while playing sports, or perhaps, from tripping. There is a vigorous contraction of the muscle and the tendon tears. Causes The tendon is susceptible to injury and can rupture during vigorous activities such as running and jumping. Rupture can also occur as a result of gradual wear. After becoming chronically weakened, it can rupture during non-stress activities like walking. Symptoms A sudden and severe pain may be felt at the back of the ankle or calf, often described as "being hit by a rock or shot" or "like someone stepped onto the back of my ankle." The sound of a loud pop or snap may be reported. A gap or depression may be felt and seen in the tendon about 2 inches above the heel bone. Initial pain, swelling, and stiffness may be followed by bruising and weakness. The pain may decrease quickly, and smaller tendons may retain the ability to point the toes. Without the Achilles tendon, though, this would be very difficult. Standing on tiptoe and pushing off when walking will be impossible. A complete tear is more common than a partial tear. Diagnosis During the physical exam, your doctor will inspect your lower leg for tenderness and swelling. In many cases, doctors can feel a gap in your tendon if a complete rupture has occurred. Achilles tendon rupture can be diagnosed reliably with clinical examination, but if there?s a question about the extent of your Achilles tendon injury then your doctor may order a magnetic resonance imaging (MRI) scan. Non Surgical Treatment Medical therapy for a patient with an Achilles tendon rupture consists of rest, pain control, serial casting, and rehabilitation to maximize function. Ongoing debate surrounds the issue of whether medical or surgical therapy is more appropriate for this injury. Conservative management of Achilles tendinosis and paratenonitis includes the following. Physical therapy. Eccentric exercises are the cornerstone of strengthening treatment, with most patients achieving 60-90% pain relief. Orthotic therapy in Achilles tendinosis consists of the use of heel lifts. Nonsteroidal anti-inflammatory drugs (NSAIDs). Tendinosis tends to be less responsive than paratenonitis to NSAIDs. Steroid injections. Although these provide short-term relief of painful symptoms, there is concern that they can weaken the tendon, leading to rupture. Vessel sclerosis. Platelet-rich plasma injections. Nitric oxide. Shock-wave therapy.  Surgical Treatment Operative treatment involves a 6cm incision along the inner side of the tendon. The torn ends are then strongly stitched together with the correct tension. After the operation a below knee half cast is applied for 2 weeks. At 2 weeks a brace will be applied that will allow you to move the foot and fully weight-bear for a further 6 weeks. After this you will need physiotherapy. Surgery carries the general risks of any operation but the risk of re-rupture is greatly reduced to 2%. The best form of treatment is controversial with good results being obtained by both methods but surgery is generally recommended for patients under 60 years of age who are fit and active with an intra-substance tear. Surgical Treatment Operative treatment involves a 6cm incision along the inner side of the tendon. The torn ends are then strongly stitched together with the correct tension. After the operation a below knee half cast is applied for 2 weeks. At 2 weeks a brace will be applied that will allow you to move the foot and fully weight-bear for a further 6 weeks. After this you will need physiotherapy. Surgery carries the general risks of any operation but the risk of re-rupture is greatly reduced to 2%. The best form of treatment is controversial with good results being obtained by both methods but surgery is generally recommended for patients under 60 years of age who are fit and active with an intra-substance tear.
|
Archives
July 2017
Categories |
 RSS Feed
RSS Feed
